COVID-19 VACCINE MANDATES:
21 Scientific Facts That
Challenge the Assumptions

 ASSUMPTION: The COVID-19 vaccines significantly reduce the spread of COVID-19, so high universal vaccination rates will prevent outbreaks.
ASSUMPTION: The COVID-19 vaccines significantly reduce the spread of COVID-19, so high universal vaccination rates will prevent outbreaks.
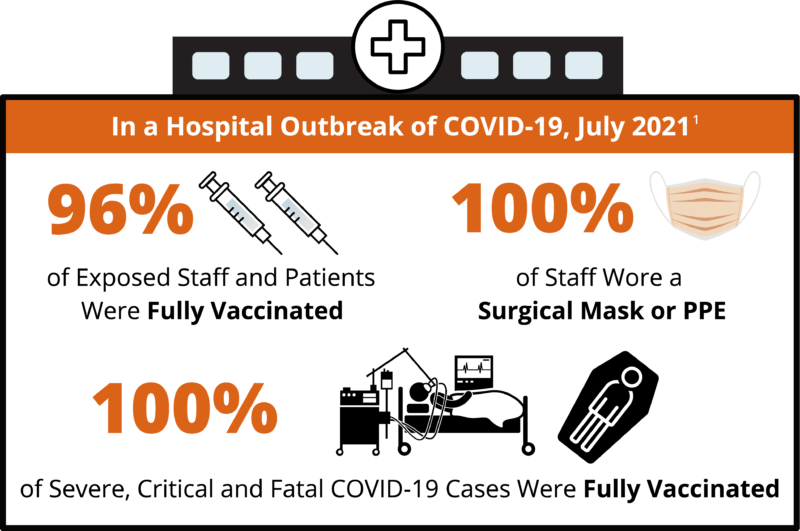
![]() FACT 1: A study of a COVID-19 outbreak in July 2021 published in Eurosurveillance found that “all transmissions between patients and staff occurred between masked and vaccinated individuals, as experienced in an outbreak from Finland.” The authors state that the study “challenges the assumption that high universal vaccination rates will lead to herd immunity and prevent COVID-19 outbreaks.”1
FACT 1: A study of a COVID-19 outbreak in July 2021 published in Eurosurveillance found that “all transmissions between patients and staff occurred between masked and vaccinated individuals, as experienced in an outbreak from Finland.” The authors state that the study “challenges the assumption that high universal vaccination rates will lead to herd immunity and prevent COVID-19 outbreaks.”1
![]() FACT 2: A Centers for Disease Control and Prevention (CDC) study of another COVID-19 outbreak in July 2021 found that 74% of cases were fully vaccinated.2
FACT 2: A Centers for Disease Control and Prevention (CDC) study of another COVID-19 outbreak in July 2021 found that 74% of cases were fully vaccinated.2
![]() FACT 3: A Harvard study investigating COVID-19 cases across 68 countries and across 2,947 counties in the U.S. found “no significant signaling of COVID-19 cases decreasing with higher percentages of population fully vaccinated.”3
FACT 3: A Harvard study investigating COVID-19 cases across 68 countries and across 2,947 counties in the U.S. found “no significant signaling of COVID-19 cases decreasing with higher percentages of population fully vaccinated.”3

A study of a COVID-19 outbreak in July 2021 found that all transmissions between patients and staff occurred between vaccinated individuals.
A Harvard study investigating COVID-19 cases across 68 countries and 2,947 counties in the U.S. found no decrease in cases with an increase in vaccination.
ASSUMPTION: The COVID-19 vaccines prevent death from COVID-19.
![]()
FACT 4: Clinical trials have observed tens of thousands of subjects and are the only studies 1) that included a control group and 2) where all subjects were monitored and tested for COVID-19 regardless of vaccination status. However, those trials did not detect enough COVID-19 deaths to measure a significant difference in mortality between vaccinated and unvaccinated patients.4-7 The U.S. Food and Drug Administration (FDA) states, “A larger number of individuals at high risk of COVID-19 and higher attack rates would be needed to confirm efficacy of the vaccine against mortality.”4-7
![]()
FACT 5: A study of a COVID-19 outbreak in July 2021 published in Eurosurveillance observed that 100% of severe, critical, and fatal cases of COVID-19 occurred in vaccinated individuals.1
![]()
FACT 6: CDC data show mass vaccination with the COVID-19 vaccine has had no measurable impact on the COVID-19 mortality rate in the U.S. In the nine months before the introduction of mass vaccination (April 2020 through December 2020), there were about 356,000 COVID-19 deaths or 39,500 deaths per month — a mortality rate of 0.120 per 1,000 people. In the nine months after the introduction of mass vaccination (January 2021 through September 2021), there were 342,000 COVID-19 deaths or 38,000 deaths per month — a mortality rate of 0.115 per 1,000 people. And in the five months that followed (October 2021 through February 2022), there were an additional 249,000 COVID-19 deaths or 49,800 deaths per month — a mortality rate of 0.151 per 1,000 people.7
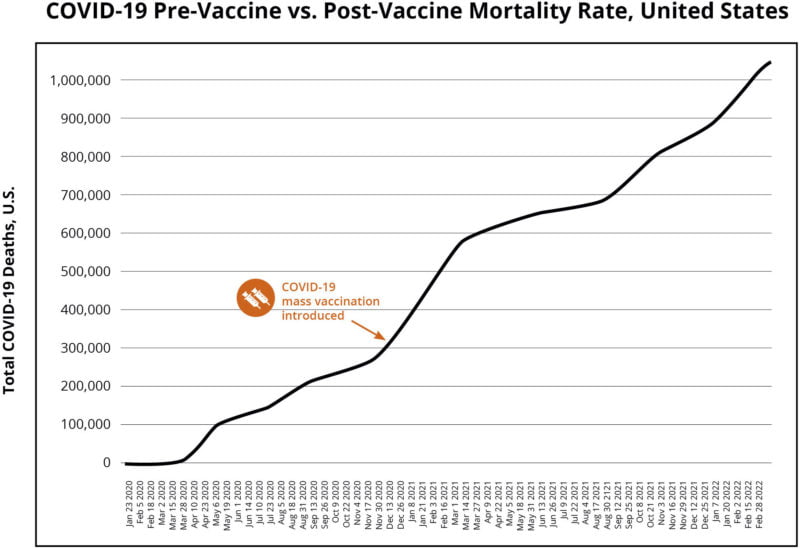
CDC data show mass vaccination with the COVID-19 vaccine has had no measurable impact on the COVID-19 mortality rate in the U.S.
ASSUMPTION: COVID-19 vaccines cause fewer hospitalizations than COVID-19.
![]()
FACT 7: A study published in Vaccine observed a risk of a serious adverse event (SAE) from the Pfizer vaccine in 1 in 556 vaccinated subjects. The same study also observed a risk of an SAE from the Moderna vaccine in 1 in 1,408 vaccinated subjects. The study states, “An SAE was defined as an adverse event that results in any of the following conditions: death; life-threatening at the time of the event; inpatient hospitalization or prolongation of existing hospitalization; persistent or significant disability/incapacity; a congenital anomaly/birth defect; medically important event, based on medical judgment.”8
In addition, the study found, “In the Moderna trial, the excess risk of serious AESIs [adverse events of special interest] (15.1 per 10,000 participants) was higher than the risk reduction for COVID-19 hospitalization relative to the placebo group (6.4 per 10,000 participants). In the Pfizer trial, the excess risk of serious AESIs (10.1 per 10,000) was higher than the risk reduction for COVID-19 hospitalization relative to the placebo group (2.3 per 10,000 participants).”8
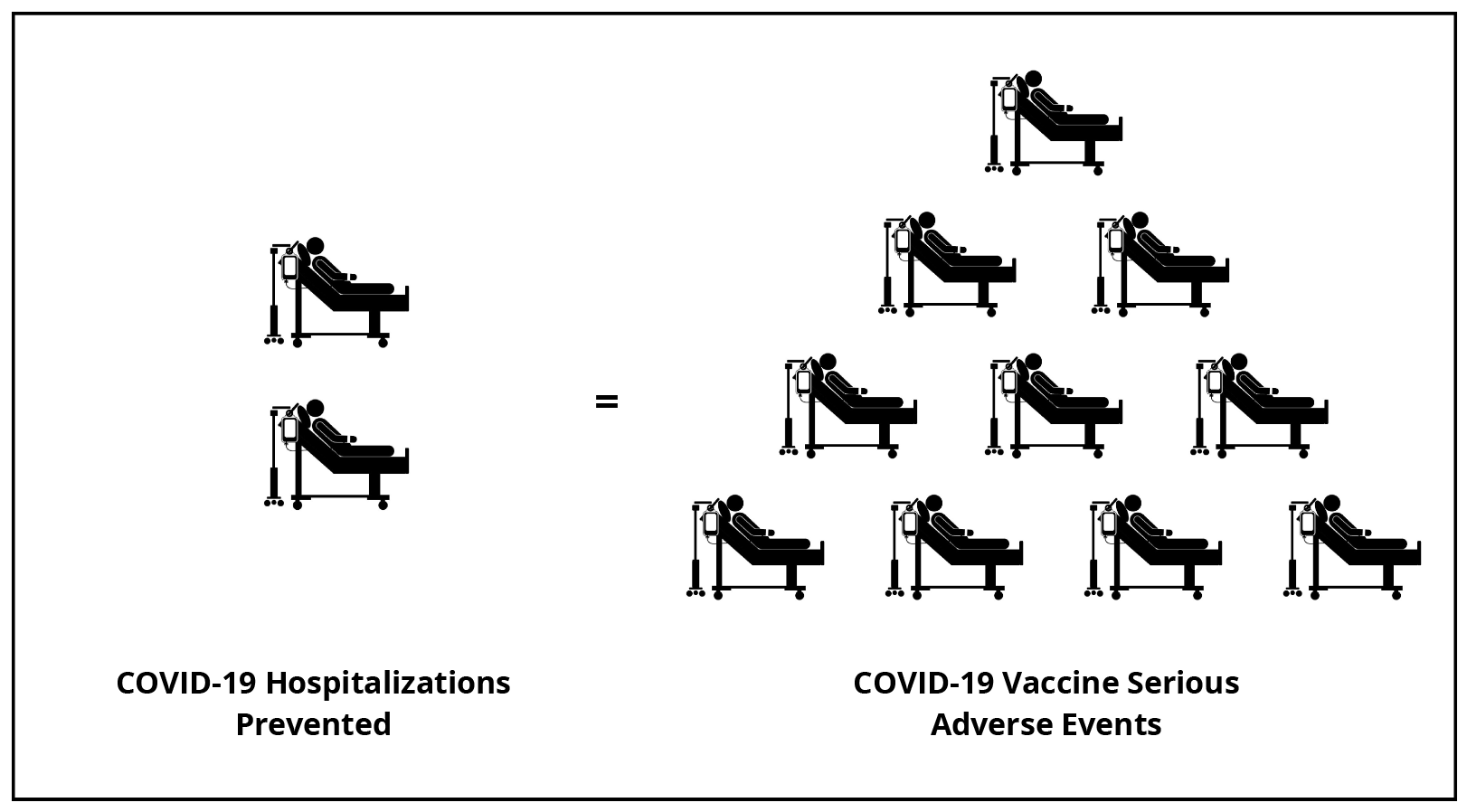
A study published in Vaccine8 found that in the Pfizer trial, the number of serious adverse events in vaccinated people was higher than the number of COVID-19 hospitalizations prevented. For every two COVID-19 hospitalizations prevented in vaccinated people, there were 10 COVID-19 vaccine serious adverse events.
ASSUMPTION: For children, being injected with COVID-19 vaccines is safer than being infected with SARS-CoV-2.
![]()
FACT 8: In the Pfizer clinical trial, there were zero cases of severe COVID-19 in children who did not receive the vaccine.9,10 In contrast, for children 5 years or older, the Pfizer COVID-19 vaccine clinical trial found that the vaccine causes severe (grade 3) systemic reactions that include fever greater than 102.1° F; vomiting that requires IV hydration; diarrhea of six or more loose stools in 24 hours; and severe fatigue, severe headache, severe muscle pain, or severe joint pain that prevents daily activity.10-13
![]()
FACT 9: In the clinical trial, a range of 1 in 59 to 1 in 143 vaccinated children 5 to 11 years of age suffered severe systemic reactions within seven days of the second dose. There were 3 to 8 cases of severe systemic reactions observed in the vaccinated group for every 10 cases of non-severe COVID-19 in the unvaccinated group.10
![]()
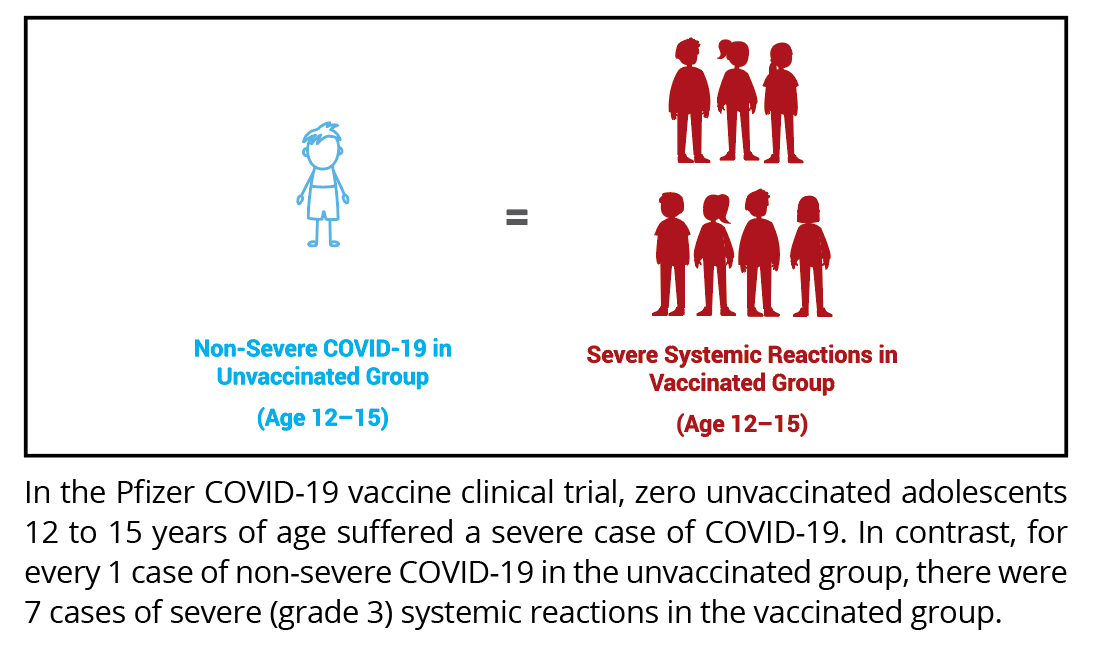
FACT 10: In the clinical trial, 1 in 9 vaccinated adolescents 12 to 15 years of age suffered severe systemic reactions within seven days of receiving the second dose. There were 7 times more severe systemic reactions observed in the vaccinated group than non-severe COVID-19 cases in the unvaccinated group.11-13
![]()
FACT 11: The clinical trial also found that 1 in about 1,100 vaccinated children 12 to 15 years of age had a grade 4 systemic reaction (fever greater than 104° F) after the first dose that required an emergency room (ER) visit and withdrawal from the study.11,12
ASSUMPTION: The COVID-19 vaccine clinical trial was large enough to show safety in children.
![]()
FACT 12: The Pfizer clinical trial did not have enough statistical power to show the vaccine is safe in children under 18 years of age, as the study did not include enough subjects to establish safety (i.e., the clinical trial only included about 2,600 vaccinated children aged 5 to 15).10,14 In comparison, it is known that COVID-19 fatalities are rare in children. Between 2020 and 2022, the chance of a child 17 years or younger contracting SARS-CoV-2 and dying from COVID-19 was 1 in 70,000 or 0.001%.15
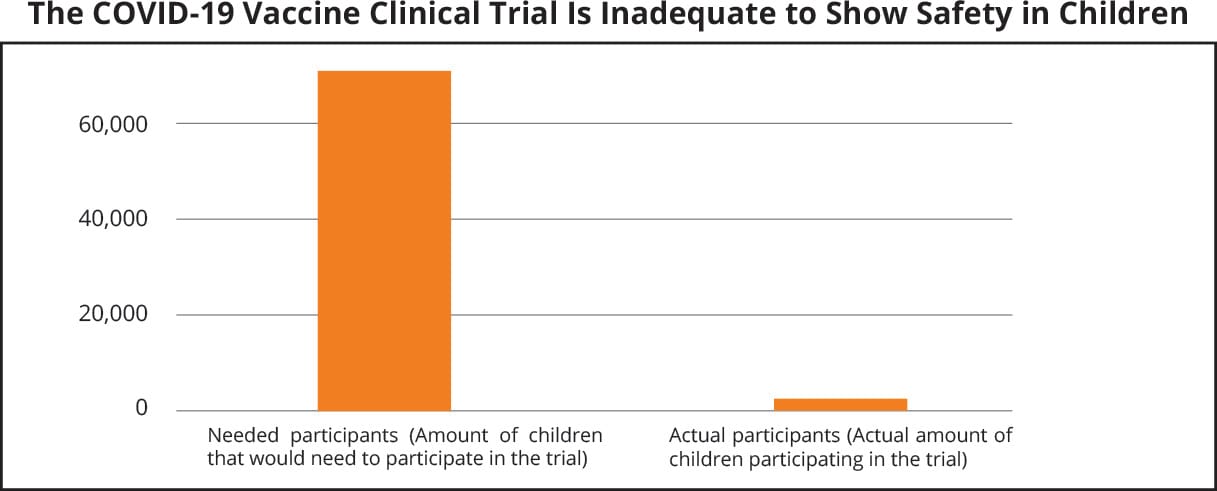
There are not enough children in clinical trials to prove that COVID-19 vaccines pose less risk than COVID-19 for children under 18 years of age.
ASSUMPTION: COVID-19 vaccines have no serious or long-term side effects.
![]()
FACT 13: Because all subjects in clinical trials were observed for only two to six months, the long-term safety of COVID-19 vaccines for any age group is not known. Per the FDA, there are currently insufficient data to make conclusions about the safety of COVID-19 vaccines in subpopulations such as pregnant and lactating individuals, and immunocompromised individuals.4,9 Per Pfizer, the vaccine “has not been evaluated for the potential to cause carcinogenicity, genotoxicity, or impairment of male fertility.”16
![]()
FACT 14: Safety surveillance reports have identified serious risks of myocarditis and pericarditis in subjects under age 40, within seven days of vaccination. In males aged 18 to 24 years, a study published in Pharmacoepidemiology and Drug Safety observed a risk of myocarditis of 1 in 1,862 after the second dose of a COVID-19 mRNA vaccine.17 In addition, a study conducted by the Florida Department of Health found a 97% increased risk of cardiac-related deaths in males aged 18–39 within 28 days of being vaccinated with a COVID-19 vaccine.18 In women, a study published in BMJ found that vaccination with two doses within the same menstrual cycle led to a 3.7-day increase in that cycle. The consequences of that phenomenon are not known.19

ASSUMPTION: Booster shots will solve the problem of waning vaccine immunity.
![]()
FACT 15: The clinical trials detected that vaccine immunity wanes significantly over a short period of time. For example, the Pfizer vaccine efficacy decreased by 8% to 18% within only six months.20 Additionally, the efficacy measured in the clinical trials was against the original Wuhan strain, not the new variants.
![]()
FACT 16: In clinical trials, a third dose of Pfizer or Moderna vaccine has not been evaluated for efficacy against disease, but rather antibody counts were observed in a small number of vaccinated subjects for only one month.21,22
ASSUMPTION: There are no known effective treatment or prevention options for COVID-19 except vaccines.
![]()
FACT 17: Treatments for COVID-19 have improved significantly since the pandemic began in early 2020, resulting in improved survival rates in hospitalized cases.23,24 Indeed, for people not living in a nursing home, the overall survival rate of COVID-19 is 99.8% in the U.S., and 99.997% for children specifically.25,26
![]()
FACT 18: Many studies have observed the effectiveness of various treatments, the most studied being ivermectin, vitamin D, hydroxychloroquine (HCQ), and monoclonal antibodies.27,28 These treatments may also be beneficial for prophylaxis (i.e., pre-exposure or post-exposure prevention of symptomatic COVID-19 infections).29-33

Treatments for COVID-19 have improved significantly since the pandemic began in early 2020, resulting in improved survival rates in hospitalized cases.

For people not living in a nursing home, the overall survival rate of COVID-19 is 99.8%, and 99.997% for children specifically.
ASSUMPTION: People who were previously infected with SARS-CoV-2 need to get vaccinated because natural immunity is insufficient.
![]()
FACT 19: There is evidence that previous SARS-CoV-2 infection is more effective at preventing SARS-CoV-2 infection than COVID-19 vaccines. An article published in Science in August 2021 states, “Newly released data show people who once had a SARS-CoV-2 infection were much less likely than never-infected, vaccinated people to get Delta, develop symptoms from it, or become hospitalized with serious COVID-19.” The article also states, “It’s a textbook example of how natural immunity is really better than vaccination.”34
![]()
FACT 20: Data from the Johnson & Johnson clinical trial also indicate that an unvaccinated person previously infected with SARS-CoV-2 has a 99.9% chance of being protected from a repeat infection.35

The Johnson & Johnson vaccine clinical trial found there are 6 times more cases of COVID-19 in vaccinated subjects than in unvaccinated subjects previously infected with SARS-CoV-2.
ASSUMPTION: Vaccine mandates have been proven to create a safer environment.
![]()
FACT 21: Infection and transmission of SARS-CoV-2 occur at high rates in fully vaccinated populations, and a significant proportion of severe, critical and fatal COVID-19 cases occur in fully vaccinated individuals. CDC data show mass vaccination with the COVID-19 vaccine has had no measurable impact on COVID-19 mortality in the U.S. In addition, short-term clinical trial data indicate that 1 in 6 to 1 in 9 people 12–55 years of age who receive mRNA COVID-19 vaccines suffer severe (grade 3) systemic reactions, and long-term safety studies have not been conducted.36 Thus, the scientific data demonstrate that vaccine mandates have not been proven to create a safer environment.
REFERENCES
Shitrit P, Zuckerman NS, Mor O, Gottesman BS, Chowers M. Nosocomial outbreak caused by the SARS-CoV-2 Delta variant in a highly vaccinated population, Israel, July 2021. Euro Surveill. 2021 Sep;26(39). https://pubmed.ncbi.nlm.nih.gov/34596015/.
Brown CM, Vostok J, Johnson H, Burns M, Gharpure R, Sami S, Sabo RT, Hall N, Foreman A, Schubert PL, Gallagher GR, Fink T, Madoff LC, Gabriel SB, MacInnis B, Park DJ, Siddle KJ, Harik V, Arvidson D, Brock-Fisher T, Dunn M, Kearns A, Laney AS. Outbreak of SARS-CoV-2 infections, including COVID-19 vaccine breakthrough infections, associated with large public gatherings—Barnstable County, Massachusetts, July 2021. MMWR Morb Mortal Wkly Rep. 2021 Aug 6;70(31):1059-62. https://www.cdc.gov/mmwr/volumes/70/wr/mm7031e2.htm?s_cid=mm7031e2_w.
Subramanian SV, Kumar A. Increases in COVID-19 are unrelated to levels of vaccination across 68 countries and 2947 counties in the United States. Eur J Epidemiol. 2021 Sep 30:1-4. https://pubmed.ncbi.nlm.nih.gov/34591202/.
U.S. Food and Drug Administration, Vaccines and Related Biological Products Advisory Committee. FDA briefing document: Moderna COVID-19 vaccine. Vaccines and Related Biological Products Advisory Committee Meeting: December 17, 2020. https://www.fda.gov/media/144434/download.
U.S. Food and Drug Administration, Vaccines and Related Biological Products Advisory Committee. FDA briefing document: Janssen Ad26.COV2.S vaccine for the prevention of COVID-19. Vaccines and Related Biological Products Advisory Committee Meeting: February 26, 2021. Table 22: vaccine efficacy of first occurrence of moderate to severe/critical and severe/critical COVID-19 including non-centrally confirmed cases with onset at least 14 or at least 28 days after vaccination, by country of participation, per-protocol set, study 3001; 37. https://www.fda.gov/media/146217/download.
U.S. Food and Drug Administration, Vaccines and Related Biological Products Advisory Committee. FDA briefing document: Pfizer-BioNTech COVID-19 vaccine. Vaccines and Related Biological Products Advisory Committee Meeting: December 10, 2020. https://www.fda.gov/media/144245/download.
Centers for Disease Control and Prevention. Washington, D.C.: U.S. Department of Health and Human Services. COVID data tracker: trends in number of COVID-19 cases and deaths in the US reported to CDC, by state/territory; [cited 2022 Apr 2]. https://covid.cdc.gov/covid-data-tracker/#trends_totaldeaths.
Fraiman J, Erviti J, Jones M, Greenland S, Whelan P, Kaplan RM, Doshi P. Serious adverse events of special interest following mRNA COVID-19 vaccination in randomized trials in adults. Vaccine. 2022 Sep 22;40(40):5798-805. https://pubmed.ncbi.nlm.nih.gov/36055877/.
U.S. Food and Drug Administration, Center for Biologics Evaluation and Research (CBER) Office of Vaccines Research and Review (OVRR). Washington, D.C.: U.S. Department of Health and Human Services. Emergency use authorization (EUA) amendment for an unapproved product: review memorandum; 2021 Apr 9: 23, 39. https://www.fda.gov/media/148542/download.
U.S. Food and Drug Administration, Vaccines and Related Biological Products Advisory Committee. FDA briefing document: EUA amendment request for Pfizer-BioNTech COVID-19 vaccine for use in children 5 through 11 years of age. Vaccines and Related Biological Products Advisory Committee Meeting: October 26, 2021. https://www.fda.gov/media/153447/download.
Wallace M. Grading of recommendations, assessment, development, and evaluation (GRADE): Pfizer-BioNTech COVID-19 Vaccine. COVID-19 Vaccines Work Group of the Advisory Committee on Immunization Practices (ACIP). Centers for Disease Control and Prevention. 2021 May 12: 24, 25. https://physiciansforinformedconsent.org/wallace-cdc-grade-pfizer-biontech-covid-19-vaccine.
Centers for Disease Control and Prevention. Washington, D.C.: U.S. Department of Health and Human Services. Grading of recommendations, assessment, development, and evaluation (GRADE): Pfizer-BioNTech COVID-19 vaccine for persons aged 12-15 years; [cited 2021 May 14]. https://physiciansforinformedconsent.org/cdc-grade-pfizer-biontech-covid-19-vaccine-12-15-years/.
Pfizer. New York (NY): Pfizer Inc. Fact sheet for healthcare providers administering vaccine (vaccination providers); revised 2021 Nov 19. Table 11: vaccine efficacy – first COVID-19 occurrence from 7 days after dose 2: without evidence of infection and with or without evidence of infection prior to 7 days after dose 2 – blinded placebo-controlled follow-up period, adolescents 12 through 15 years of age evaluable efficacy (7 days) population; 48. https://physiciansforinformedconsent.org/pfizer-fact-sheet-for-healthcare-providers-administering-vaccine.
Pfizer. New York (NY): Pfizer Inc. Fact sheet for healthcare providers administering vaccine (vaccination providers); revised 2021 Nov 19: 48. https://physiciansforinformedconsent.org/pfizer-fact-sheet-for-healthcare-providers-administering-vaccine.
Centers for Disease Control and Prevention. Washington, D.C.: U.S. Department of Health and Human Services. CDC wonder: about underlying cause of death, 2018-2022, single race; [cited 2024 August 8]. https://wonder.cdc.gov/ucd-icd10-expanded.html. Query for COVID-19 deaths of age 17 or younger, 2020-2022.
Pfizer. New York (NY): Pfizer Inc. Comirnaty (COVID-19 vaccine, mRNA) suspension for injection, for intramuscular use; revised 2021 Dec. https://www.fda.gov/media/151707/download.
Sharff KA, Dancoes DM, Longueil JL, Johnson ES, Lewis PF. Risk of myopericarditis following COVID-19 mRNA vaccination in a large integrated health system: a comparison of completeness and timeliness of two methods. Pharmacoepidemiol Drug Saf. 2022 Aug;31(8):921-5. https://pubmed.ncbi.nlm.nih.gov/35404496/.
Florida Department of Health. Exploring the relationship between all-cause and cardiac-related mortality following COVID-19 vaccination or infection in Florida residents: a self-controlled case series study; [cited 2022 Oct 13]. https://physiciansforinformedconsent.org/fl-dept-health-cardiac-related-mortality-following-COVID-19-vaccination/.
Edelman A, Boniface ER, Male V, Cameron ST, Benhar E, Han L, Matteson KA, Van Lamsweerde A, Pearson JT, Darney BG. Association between menstrual cycle length and COVID-19 vaccination: global, retrospective cohort study of prospectively collected data. BMJ Medicine. 2022;1:e000297. https://bmjmedicine.bmj.com/content/1/1/e000297.
Thomas SJ, Moreira ED Jr, Kitchin N, Absalon J, Gurtman A, Lockhart S, Perez JL, Pérez Marc G, Polack FP, Zerbini C, Bailey R, Swanson KA, Xu X, Roychoudhury S, Koury K, Bouguermouh S, Kalina WV, Cooper D, Frenck RW Jr, Hammitt LL, Türeci Ö, Nell H, Schaefer A, Ünal S, Yang Q, Liberator P, Tresnan DB, Mather S, Dormitzer PR, Şahin U, Gruber WC, Jansen KU; C4591001 Clinical Trial Group. Safety and efficacy of the BNT162b2 mRNA covid-19 vaccine through 6 months. N Engl J Med. 2021 Nov 4;385(19):1761-73. https://pubmed.ncbi.nlm.nih.gov/34525277.
U.S. Food and Drug Administration, Vaccines and Related Biological Products Advisory Committee. FDA briefing document: Application for licensure of a booster dose for Comirnaty (COVID-19 Vaccine, mRNA). Vaccines and Related Biological Products Advisory Committee Meeting: September 17, 2021. https://www.fda.gov/media/152176/download.
U.S. Food and Drug Administration, Vaccines and Related Biological Products Advisory Committee. FDA briefing document: EUA amendment request for a booster dose for the Moderna COVID-19 vaccine. Vaccines and Related Biological Products Advisory Committee Meeting: October 14, 2021. https://www.fda.gov/media/152991/download.
Horwitz LI, Jones SA, Cerfolio RJ, Francois F, Greco J, Rudy B, Petrilli CM. Trends in COVID-19 risk-adjusted mortality rates. J Hosp Med. 2021 Feb;16(2):90-2. https://www.journalofhospitalmedicine.com/jhospmed/article/230561/hospital-medicine/trends-covid-19-risk-adjusted-mortality-rates.
Dennis JM, McGovern AP, Vollmer SJ, Mateen BA. Improving survival of critical care patients with coronavirus disease 2019 in England: a national cohort study, March to June 2020. Crit Care Med. 2021 Feb 1;49(2):209-14. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7803441/.
Ioannidis, JPA. Reconciling estimates of global spread and infection fatality rates of COVID- 19: an overview of systematic evaluations. Eur J Clin Invest. 2021;51:e13554. https://onlinelibrary.wiley.com/doi/epdf/10.1111/eci.13554.
Physicians for Informed Consent. COVID-19 — disease information statement (DIS). 2020 Jun; updated 2024 Nov. https://physiciansforinformedconsent.org/covid-19-disease-information-statement/.
C19early.com. COVID-19 early treatment: real-time analysis of 1,298 studies; [cited 2022 Jan 11]. https://c19early.com/.
U.S. Food and Drug Administration. Silver Spring (MD): U.S. Food and Drug Administration. FDA news release — FDA roundup: March 22, 2024; [cited 2024 Aug 30]. https://www.fda.gov/news-events/press-announcements/fda-roundup-march-22-2024.
C19early.com. COVID-19 studies: ivermectin; [cited 2022 Feb 12]. https://c19ivermectin.com.
Bryant A, Lawrie TA, Dowswell T, Fordham EJ, Mitchell S, Hill SR, Tham TC. Ivermectin for prevention and treatment of COVID-19 infection: a systematic review, meta-analysis, and trial sequential analysis to inform clinical guidelines. Am J Ther. 2021 Jun 21;28(4):e434-60. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8248252/.
C19early.com. COVID-19 studies: vitamin D; [cited 2022 Feb 12]. https://c19vitamind.com.
Ilie PC, Stefanescu S, Smith L. The role of vitamin D in the prevention of coronavirus disease 2019 infection and mortality. Aging Clin Exp Res. 2020 Jul;32(7):1195-8. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7202265/.
C19early.com. HCQ for COVID-19: real-time meta analysis of 303 studies; [cited 2022 Jan 10]. https://hcqmeta.com.
Wadman M. Having SARS-CoV-2 once confers much greater immunity than a vaccine — but vaccination remains vital. Science. 2021 Aug 26 [cited 2024 Sep 1]. https://www.science.org/content/article/having-sars-cov-2-once-confers-much-greater-immunity-vaccine-vaccination-remains-vital.
U.S. Food and Drug Administration, Vaccines and Related Biological Products Advisory Committee. FDA briefing document: Janssen Ad26.COV2.S vaccine for the prevention of COVID-19. Vaccines and Related Biological Products Advisory Committee Meeting: February 26, 2021. Table 14: vaccine efficacy of first occurrence of moderate to severe/critical COVID-19, including non-centrally confirmed cases, with onset at least 14 or at least 28 days after vaccination, by baseline SARS-CoV-2 status, per protocol set; 30. https://www.fda.gov/media/146217/download.
El Sahly HM, Baden LR, Essink B, Doblecki-Lewis S, Martin JM, Anderson EJ, Campbell TB, Clark J, Jackson LA, Fichtenbaum CJ, Zervos M, Rankin B, Eder F, Feldman G, Kennelly C, Han-Conrad L, Levin M, Neuzil KM, Corey L, Gilbert P, Janes H, Follmann D, Marovich M, Polakowski L, Mascola JR, Ledgerwood JE, Graham BS, August A, Clouting H, Deng W, Han S, Leav B, Manzo D, Pajon R, Schödel F, Tomassini JE, Zhou H, Miller J; COVE Study Group. Efficacy of the mRNA-1273 SARS-CoV-2 vaccine at completion of blinded phase. N Engl J Med. 2021 Nov 4;385(19):1774-85. Suppl appendix; 36-7. https://www.nejm.org/doi/suppl/10.1056/NEJMoa2113017/suppl_file/nejmoa2113017_appendix.pdf.
Published 2022 Feb; updated 2024 Nov.